


1Department of Dermatology, Ghent University Hospital, 2Faculty of Medicine and Health Science, Ghent University, Ghent, Belgium, 3Dutch Society for Vitiligo Patients (Vitiligo.NL), The Hague, 4Department of Dermatology, Institute for Pigment Disorders and Infection & Immunity Institute Amsterdam UMC, Amsterdam, The Netherlands
#These authors contributed equally and should be considered as first authors.
Identifying which factors contribute to vitiligo severity and determining their individual weight are important in the management of vitiligo. The aim of this study is to investigate the predictive variables concerning vitiligo severity as perceived by the patients. Based on a questionnaire, several factors that may contribute to the Patient Global Assessment (PtGA) of severity were investigated within a Belgian vitiligo population (n = 291). In addition, possible factors influencing vitiligo severity were scored and ranked. The strongest correlations with the PtGA of severity were found for impact, Dermatology Life Quality Index and disease extent. Based on multivariable regression analyses, 64.7% of PtGA of severity could be predicted by subjective and objective variables, while 32% could be explained by objective clinical features only. Patients considered lesion location, extent and disease activity as the most important contributing factors to severity. Vitiligo severity is determined by objective clinical features, but also, for a significant part, by the perceived impact of the disease.
Key words: vitiligo; severity; quality of life; patient-reported outcomes; impact; outcome.
Accepted May 5, 2021; Epub ahead of print May 6, 2021
Acta Derm Venereol 2021; 101: adv00481.
doi: 10.2340/00015555-3823
Corr: Nanja van Geel, Department of Dermatology, Ghent University Hospital, Corneel Heymanslaan 10, BE-9000 Ghent, Belgium. E-mail: Nanja.vangeel@UGent.be
Understanding which factors determine the severity of vitiligo from a patients’ perspective is crucial to choose the right treatment for the individual patient. Traditionally, the extent of the disease, has been considered the main factor that influences the severity of vitiligo. This study found that a combination of several objective clinical features (e.g. extent, skin type, disease activity) explains 32% of the variation in perceived disease severity, and that personal subjective factors (e.g. perceived disease impact) explain another major part. These findings are important for the management of vitiligo and stratification of patients in treatment guidelines.
Vitiligo is an acquired depigmenting skin disease affecting approximately 0.5–2% of the population worldwide. There is no definite cure to date, but available treatments have varying success (1). New and promising treatments are currently being investigated (2, 3). To develop treatment decision guidelines or criteria for these novel therapies a correct definition or interpretation of “severity” is required (4). This will not only lead to more meaningful criteria, but also to a more accurate evaluation of vitiligo status and subsequent better patient-centred care.
Severity of vitiligo is closely associated with the disease extent: the determination of the affected body surface area (BSA) is, in general, considered a relevant aspect in the assessment of vitiligo severity. For the latter, we recently developed and validated the Self Assessment Vitiligo Extent Score (SAVES) for the patient to measure the BSA affected (5). However, severity may not only entail disease extent, but also additional factors, such as disease activity, location of lesions, skin phototype, and other patient-related factors. In addition, impact on quality of life (QoL) can also significantly contribute to the perception of severity of vitiligo. It has been shown previously that QoL is related to factors such as the time of disease onset, Sex, age, cultural differences, limitations in social life and differences in coping mechanisms with the disease (e.g. anger, embarrassment, shame, depression) (6–8). Identification of such factors may aid in defining vitiligo severity, which subsequently may be integrated into treatment decisions or criteria.
Setting up these criteria only from the physician’s point of view can lead to prerequisites that leave subsets of “ineligible” patients with unmet medical needs. For psoriasis, the minimum severity for access to some biologicals is set at a Psoriasis Area Severity Index (PASI) score of 10. This restriction excludes patients with psoriasis who have solely genital, scalp or nail psoriasis, leaving them with less efficacious treatments, while the psychosocial impact may be high (9). It is therefore of primary importance to investigate the definition of disease severity of vitiligo from the patient’s point of view.
The aim of this study was to gain insight into which variables are independently associated with and predict vitiligo severity, as perceived by the patients. For this we performed a survey within a Belgium cohort inquiring into the patient’s experience of their own vitiligo and factors that might affect vitiligo severity in general.
Study design and ethics
This trial was conducted during consultations at the Department of Dermatology at the Ghent University Hospital in Belgium (October 2017 to start of October 2019). The questionnaire was constructed in cooperation with the Dutch society for vitiligo patients “Vitiligo.nl” and in collaboration with Amsterdam University Medical Center (the Netherlands). The study was approved by the local ethics committees of Ghent University Hospital and reported at the Amsterdam Medical Center (reference numbers: B670201421409 and W17_355#17.413 respectively). Written informed consent from all participants completing the questionnaire was requested. The COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) checklist was used as a guidance for designing and reporting the study.
Participants
Participants were vitiligo (non-segmental) patients ≥ 16 years of age consulting the Department of Dermatology at Ghent University Hospital (Belgium), who were willing to complete the questionnaire.
Construction of the questionnaire
A draft version of the questionnaire was thoroughly checked by several members of the Dutch patient society (vitiligo.nl) and modified based on patients’ preferences. Validation (content and construct validity) of the used Patient Global Assessment (PtGA) of severity (5 point scale) and the Impact score (scale 0–10) and their exact formulations are described in our previous paper (10). The PtGA is based on a 5-point rating scale (ranging from very severe to not severe at all) and is introduced by a question on how the patients perceive the overall severity of their vitiligo when considering all factors, such as vitiligo extent, skin type, lesion location, etc. The content validity (relevance, completeness and comprehensiveness) of the remaining questions included in this study was also evaluated by the same members of the Dutch patient society.
The questionnaire was divided into 2 parts: Part 1 included patients’ characteristics (e.g. disease extent, skin phototype, age of onset, associated thyroid disease, disease activity) and individual/personal interpretation of their vitiligo severity (PtGA of severity) and impact. Location-related variables (presence and extent of lesions on visible areas (face and hands) were assessed with the SAVES. Part 2 focused on the patients’ interpretation of contributing factors to vitiligo severity in general. Potential factors associated with vitiligo severity in general were rated by the patients on a scale from 0 to 10. These potential factors were chosen a priori by the patients’ panel involved in construction of the questionnaire. Factors included were: vitiligo extent, impact on daily life, location of vitiligo, age, sex, photo skin type, country of origin/culture, activity/stability of vitiligo, reactions from other people, and modified behaviour because of vitiligo. The same 10 items were ranked in a top 5 according to the assumed contribution to the overall severity of vitiligo in general. All questionnaires were self-administered by the patients. Within a subgroup of patients (age ≥ 18 years) body locations as presented in the SAVES were ranked in order of significance.
Statistical analysis
Statistical analyses were performed using IBM SPSS® Statistics version 26 (SPSS Science, Chicago, IL, USA). Descriptive statistical analysis was performed for patient characteristics and responses. Linear regression analyses were carried out to determine the association between variables included in the study and the PtGA of severity. The strength of the correlation between the variables and the PtGA of severity was evaluated with Spearman’s correlation coefficients. The adjusted R square is reported to show the proportion of explained variation in PtGA of severity. Missing values were excluded from the final analysis.
Sixteen variables were considered to be interesting to investigate and were selected a priori (pre-specified variables) and included in the correlation and regression analyses: SAVES score (total disease extent), number of locations involved, disease activity in the past 6 months, number of active locations, disease duration, skin type, extent and presence of vitiligo on visible areas (hand or face), age at inclusion, sex, associated thyroid disease, age of disease onset, impact score and Dermatology Life Quality Index (DLQI).
A full model was constructed and automatic backwards multivariable regression analyses performed, assuming linear relationships of predictors to outcome (p-value < 0.1). Only variables that were significantly associated (p < 0.05) with PtGA of severity in the univariable regression analysis were included in the final model (Table SI). Disease impact and DLQI were regarded as composite measures including aspects of disease extent, disease activity, and location of the lesions. Therefore, regression analyses with and without disease impact and DLQI were performed. In the case of multicollinearity, the variable with the lowest R2 in the univariate regression was excluded. The ranking scores for contributing factors to vitiligo severity in general were compared with the paired samples Wilcoxon test. Comparisons between groups were conducted using the Kruskal–Wallis test. All tests were 2-sided, and the significance level was set at 5%.
Patients characteristics in relation to the Patient Global Assessment of severity
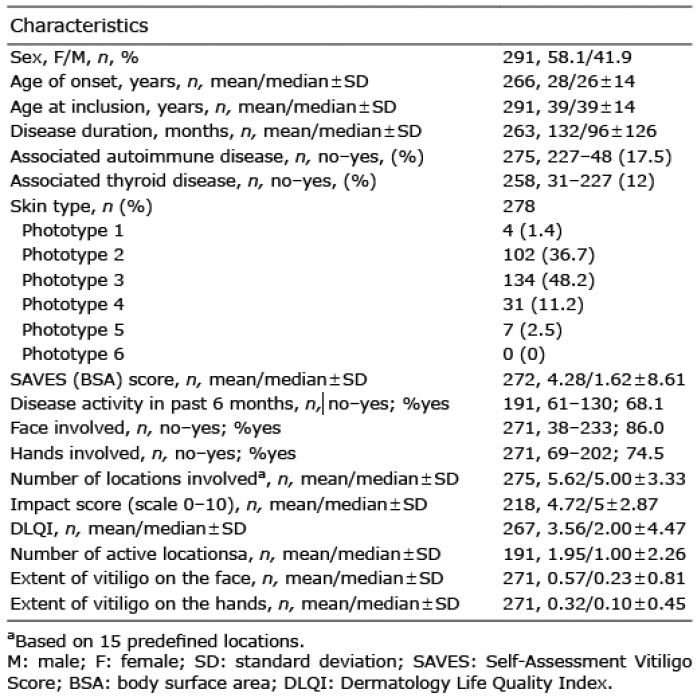
In total, 315 patients were recruited from Ghent University Hospital. Of those, a total of 291 completed the PtGA question about severity and could be used for further analyses (Table I). Patient clinical features/characteristics (e.g. age, sex, skin phototype, vitiligo extent, disease activity, disease duration, presence of lesions on hand and face) and quality of life-related outcome measures (e.g. Impact scale 0–10 and DLQI) are shown in Table I. Fig. 1 includes the general distribution of the PtGA of severity within our population.
Table I. Patients’ characteristics
Fig. 1. General distribution of the Patient Global Assessment (PtGA) of severity scores.
Univariable linear regression and correlation analysis
This part investigated the contribution of the different clinical variables and quality of life-related outcome measures to the PtGA of severity. Based on the univariate linear regression analyses shown in Table SII, it is demonstrated how much the variation (R2) in the patients’ severity perception can be explained/predicted by each separate variable. Highest adjusted R² scores were found for impact score 0–10, DLQI, vitiligo extent, extent of vitiligo on the hands and number of locations involved (adjusted R2 0.513, R2 0.251, R2 0.107, R2 0.099 and R2 0.095, respectively (p < 0.001)), while moderate associations were found for the presence of vitiligo on the hands, the extent of vitiligo on the face, number of active locations, disease activity in the last 6 months, disease duration, skin type and age at inclusion (adjusted R2 0.065, R2 0.063, R2 0.051, R2 0.031, R2 0.036, R2 0.018, and R2 0.015 respectively). The adjusted R² of vitiligo extent on visible areas (hands and face) contributed more to the PtGA of severity than just the presence or absence of vitiligo on these locations. The significant variables in this univariate regression model were subsequently included in the multivariate regression model.
Spearman’s correlation analysis demonstrated that the PtGA of severity showed the highest correlations with Impact 0–10 (r = 0.71), DLQI (r = 0.49), vitiligo extent (r = 0.44) and vitiligo extent on the hands (r = 0.35) and moderate correlations with disease activity (1: activity in past 6 months (r = 0.20); and 2: number of active locations (r = 0.22)).
Multivariable linear regression analyses
Based on the multivariable linear regression models (Table II), it is demonstrated that 5 independent variables remain significant in the regression model based on backwards selection: Impact scale 0–10, skin phototype, vitiligo extent, presence of vitiligo on the hands, and extent of vitiligo on the face. However, disease impact is a composite measure influenced by several disease-related factors. In a multiple regression model excluding Impact 0–10 and DLQI, 4 independent clinical features explain 32% (adjusted R² 0.320) of the variance of PtGA of severity: vitiligo extent, extent of lesions on the face, disease activity (number of active locations) and skin phototype.
Table II. Multiple linear regression models
After the addition of the disease impact score 0–10 and, in a second step, DLQI, the explained variation increased to 62.8% and 63.3%, respectively, indicating that the DLQI accounted for only an additional R2 of 0.005 independent of disease impact. This indicates that impact measures almost all aspects of DLQI that contribute to PtGA of severity. Nonetheless, no evidence of multicollinearity was found for DLQI and impact score (0–10) in the regression model (variance inflation factor (VIF): 1.85 and 1.72, respectively and tolerance: 0.54 and 0.5, respectively) indicating that both scores also measure, to some extent, a slightly different part of the disease. After the addition of the disease impact score 0–10 and DLQI, the independent factors for the explained variation (64.7%) did not withhold the DLQI in the final backward regression model.
Factors influencing vitiligo severity in general according to the patients
In Part 2, patients were asked about their opinion on which factors of the disease they believed influence the general severity of vitiligo the most. A score (of 0–10) for the contribution of each separate factor to vitiligo severity in general (not referring to patients’ individual situations) was asked (Table III). Median scores higher than 6 were attributed to lesion location (median 8; interquartile range (IQR) 6–10), disease extent (median 8; IQR 5–10), disease activity (median 7; IQR 5–9) and reactions from the patients’ environment (median 7; IQR 4–9). Notably, the location of lesions had a higher mean ranked score than the disease extent (Table SII; p-value from Wilcoxon signed-rank test < 0.001). It was also noted that the activity/stability of the disease had a higher median ranked score (median 7; IQR 5–9) than daily impact (median 6; IQR 3–8), modified behaviour (median 6; IQR 1–9), skin phototype (median 5; IQR 2–8), age (median 5; IQR 2–7), sex (median 3; IQR 0–5) and cultural background (median 2; IQR 0–6) (p-values < 0.01).
When patients were asked to rank the same 10 items in a top 5 according to relevance in the contribution to severity perception, the highest ranks were observed for the location of lesions (ranked in top 1: 41.5%, ranked in top 1–3: 80.3%), followed by disease extent (ranked in top 1: 32.5%, ranked in top 1–3:74.7%) disease impact (ranked in top 1: 9.8%, ranked in top 1–3: 47.2%) and disease activity (ranked in top 1: 5.7%, ranked in top 1–3: 30.1%) (Table III).
Table III. Ranking factors in top 3 of 5 selected factors
Ranking body locations according to their importance in the context of severity perception
Fifty patients (age range 18–69 years) ranked the body locations (1 as most important and 15 as the least important body location) (Table IV). Significant higher ranks were found for the face, followed by the hands, arms, trunk and legs. The back, feet, armpits, genital and gluteal area were considered to be less important locations contributing to severity perception in general.
Table IV. Body locations ranked according to the importance (interpretation of vitiligo severity in general)
This study evaluated potential factors associated with perception of vitiligo severity. A commonly used assessment method to evaluate vitiligo from the physician’s point of view is disease extent. In clinical practice and trials, the use of scoring systems to estimate disease extent, such as the Vitiligo Extent Score or Vitiligo Area Scoring Index, remain important, as they provide key information about the status of the disease and quantify differences over time (11, 12). However, this information will not necessarily reflect the disease severity as experienced by the patient.
Previously, we confirmed the validity of the PtGA score for assessing vitiligo severity (10). In the current study we identified several independent factors (impact, skin phototype, extent, presence of vitiligo on the hands, extent of lesions on the face and hands) contributing for 65% of the variance in the PtGA for disease severity as experienced by the patients. A model including only objective clinical features (excluding impact and DLQI) resulted in an explained variance of 32%, including the independent factors disease extent, skin phototype, number of active locations and extent of lesions in the face. The finding that the PtGA of severity is, for a large part, not explained by measurable physical characteristics stresses the fact that physicians are unable to correctly classify the severity of vitiligo as experienced by the patient based on clinical disease criteria alone. Impact scales, whether it is a short 0–10 scale, as used in the current study, or detailed questionnaires, such as the Vitiligo Impact Patient Scale (VIPs), offer crucial additional information to estimate the perceived severity of the disease (13, 14). Separating the subjective (e.g. perceived disease impact) from clinical components (objective clinical features) of disease severity can help to design and justify the optimal treatment strategy. Furthermore, it will lead to an increased individual treatment approach and facilitate personalized advice on coping strategies for patients with vitiligo (15).
An interesting finding was that the extent of vitiligo on visible areas (hands and face) contributed more to the PtGA of severity than just the presence or absence of vitiligo on these locations. This was also reflected in the significant correlations found in the current study between the extent of vitiligo on the hands and face (r = 0.34 and r = 0.22) and PtGA of severity. Moreover, in Part 2 of this study, both the location and extent of the lesions were ranked by the patients on top as the most important factor contributing to vitiligo severity in general.
Disease activity (number of active locations) was withheld as a significant independent predictive factor for disease severity (PtGA of severity) in the multivariable regression analyses excluding impact and DLQI. Although active vitiligo, in most cases, lacks pruritus or pain, disease activity in this study is also clearly linked with perceived severity of vitiligo. This was demonstrated by the significant correlations between the 2 disease activity scores (activity in the past 6 months and number of active locations) and the PtGA of severity. Disease stability is often neglected as a primary outcome in studies, and long-term data on the best strategy to limit disease progression are limited. This is important, as disease stability is a more feasible treatment target with the currently available treatments, while > 75% repigmentation (primary outcome in the Cochrane review) is less often achieved (16).
Strengths and limitations
The strengths of this study are the large patient population, and that the questionnaire was constructed in cooperation with the Dutch society for vitiligo patients to ensure content validity. To our knowledge, no similar data have been published to date in the field of vitiligo. However, some limitations of this study should be noted. First, no generalization of results is yet possible, due to the recruitment at only a single tertiary referral centre. Further trials are needed to confirm the results in different patient populations including more patients with skin phototype IV–VI. Another limitation is that we considered only 2 unique locations (face and hands) based on the a priori assumption that these visible locations may contribute the most to the perceived disease severity. Regarding perception of severity (PtGA of severity), post-hoc partial correlations controlled for disease extent (SAVES) showed correlation coefficients for the extent of vitiligo on the hands, the face, the trunk, the extremities, and the feet of 0.153 (p < 0.012), 0.101 [p = not significant (NS)], –0.113 (p = NS), 0.033 (p = NS), and –0.001 (p = NS), respectively.
Conclusion
This study provides important information about the perception of disease severity by patients, and represents valuable information for clinical practice and clinical trials. Furthermore, this information is essential in composing treatment criteria. Patients’ perceptions of the severity of vitiligo can be considered as a composite measure, including not only objective clinical features (e.g. disease extent), but also, for a significant part, subjective factors (e.g. perceived disease impact).
We thank all participating patients in this study and the Dutch Society for Vitiligo patients (Vitiligo.nl).
The study was approved by the local ethics committees (reference number Ghent: B670201421409; reference number Amsterdam: W15_117#15.00147).
EADV grant (EADV Project proposal reference number 2015-030), Leo Foundation grant (Leo Foundation project reference number LF16092) and grant from Incyte Bioscience. The research activities of N. van Geel are supported by the Scientific Research Foundation-Flanders (FWO Senior Clinical Investigator: 1831512N). The research activities of the R. Speeckaert are supported by the Scientific Research Foundation-Flanders (Krediet aan Navorsers: 1504718N and FWO Senior Clinical Investigator: 18B2721N).
NvG is a consultant and/or investigator for Pfizer, Laboratoire Génévrier, Incyte, Sunpharma.


 Click to show fullsize
Click to show fullsize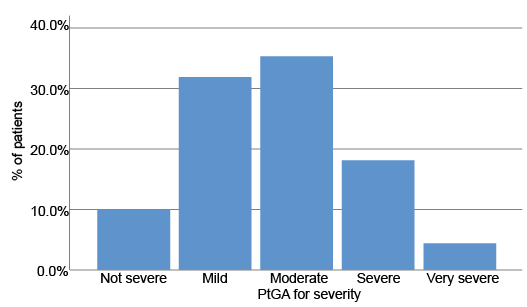 Click to show fullsize
Click to show fullsize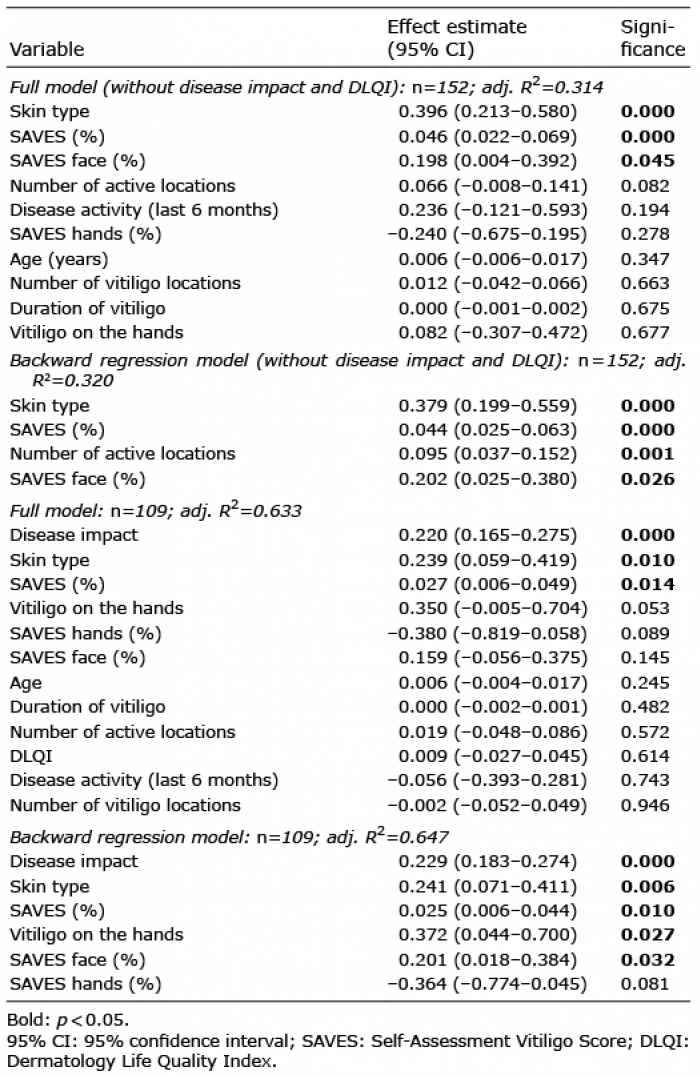 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize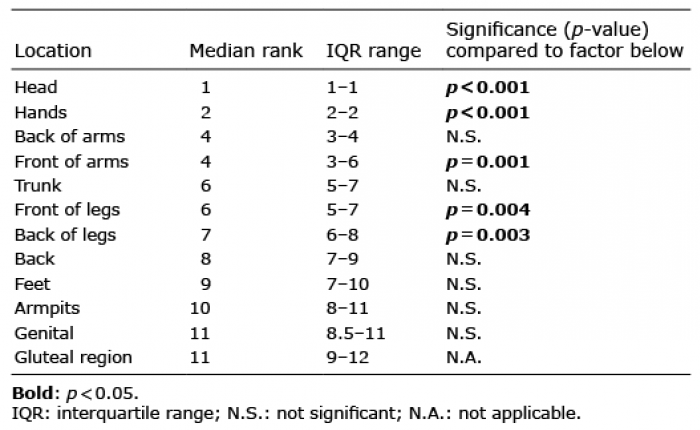 Click to show fullsize
Click to show fullsize